

Background:
Recent clinical trials have shown a steady improvement in the outcomes of patients with multiple myeloma (MM), especially in those who have received induction with bortezomib, lenalidomide, and dexamethasone (VRD), followed by autologous hematopoietic cell transplantation (Auto-HCT) and lenalidomide maintenance (Attal et al. 2017, Joseph et al. 2020). Here, we report our center's outcomes of MM patients who received VRD induction, followed by Auto-HCT and maintenance therapy incorporating lenalidomide.
Methods:
In this single-center retrospective analysis, eligible patients received an auto-HCT between June 2007 and November 2015. We excluded patients who received induction regimens other than VRD or did not receive lenalidomide-based maintenance therapy. Primary endpoints were progression-free survival (PFS) and overall survival (OS), which were estimated by using the Kaplan-Meier method. We performed multivariate Cox regression analysis to evaluate the impact of several important variables, including age, sex, race, immunoglobulin subtype, light chain, ISS, cytogenetic risk, conditioning regimen, post-transplant therapy, and best final response, on PFS and OS.
Results:
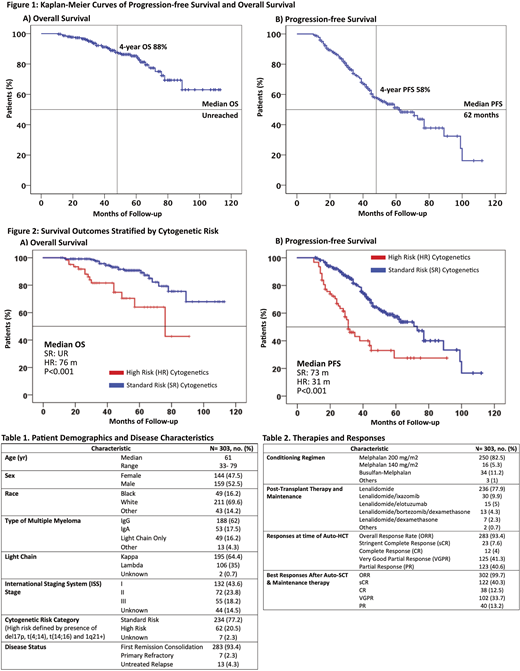
We identified 303 patients who fulfilled the eligibility criteria for this study. Table 1 and 2 summarize patient demographics, disease characteristics, therapies and responses. Sixty-two patients (20.5%) had high risk cytogenetics defined as del17p, t(4;14), t(14;16), and 1q21 gain. 132 (43.6%), 72 (23.8%), and 55 (18.2%) patients had ISS stages I, II, and III, respectively. Overall response rate (ORR) at time of Auto-HCT was 93.4% (sCR 7.6%, CR 4%, VGPR 41.3%, and PR 40.6 %). Importantly, ORR after auto-HCT and maintenance therapy was 99.7% (sCR 40.3%, CR 12.5%, VGPR 33.7%, and PR 13.2%). With a median follow up of 45 months (range: 11 - 113 months), the median PFS was 62 months (95% confidence interval (CI) 48- 76 months) and 4-year PFS was 58% (Fig 1). Median OS has not been reached and 4-year OS was 88% (Fig 1). Patients with high-risk cytogenetics had median PFS and OS of 31 months (95% CI 25- 37 months) and 76 months (95% CI 44-108 months), respectively. In contrast, in patients with standard-risk cytogenetics, the median PFS and OS were 73 months (95% CI 62- 84 months) and not reached, respectively (P<0.001; Fig 2). On multivariate analysis, standard-risk cytogenetics (P<0.001- HR 0.349, P=0.001- HR 0.278) and the final best response of >VGPR (P<0.001 - HR 0.439, P=0.001 - HR 0.306) were associated with significantly better PFS and OS, respectively.
Conclusions:
These results provide further evidence that VRD induction followed by Auto-HCT and lenalidomide-based maintenance is associated with excellent outcomes in MM, especially in patients with standard-risk cytogenetics.
Bashir:KITE: Other: Advisory Board; Celgene: Research Funding; StemLine: Research Funding; Amgen: Other: Advisory Board; Purdue: Other: Advisory Board; Takeda: Other: Advisory Board, Research Funding; Acrotech: Research Funding. Nieto:Novartis: Other: Grant Support; Astra Zeneca: Other: Grant Support; Affimed: Consultancy, Other: Grant Support; Secura Bio: Other: Grant Support. Lee:Daiichi Sankyo: Research Funding; Sanofi: Consultancy; GlaxoSmithKline: Consultancy, Research Funding; Genentech: Consultancy; Takeda: Consultancy, Research Funding; Janssen: Consultancy, Research Funding; Celgene: Consultancy, Research Funding; Regeneron: Research Funding; Genentech: Consultancy; Amgen: Consultancy, Research Funding. Patel:Celgene: Consultancy, Research Funding; Nektar: Consultancy, Research Funding; Cellectis: Research Funding; Bristol Myers Squibb: Consultancy, Research Funding; Precision Biosciences: Research Funding; Takeda: Consultancy, Research Funding; Janssen: Consultancy, Research Funding; Oncopeptides: Consultancy; Poseida: Research Funding. Kebriaei:Amgen: Other: Research Support; Kite: Other: Served on advisory board; Novartis: Other: Served on advisory board; Jazz: Consultancy; Pfizer: Other: Served on advisory board; Ziopharm: Other: Research Support. Thomas:Pharmacyclics: Other: Advisory Boards; X4 Pharma: Research Funding; Ascentage: Membership on an entity's Board of Directors or advisory committees, Research Funding; Genentech: Research Funding; Xencor: Research Funding; BMS: Research Funding. Orlowski:Sanofi-Aventis, Servier, Takeda Pharmaceuticals North America, Inc.: Honoraria, Membership on an entity's Board of Directors or advisory committees; Founder of Asylia Therapeutics, Inc., with associated patents and an equity interest, though this technology does not bear on the current submission.: Current equity holder in private company, Patents & Royalties; STATinMED Research: Consultancy; Laboratory research funding from BioTheryX, and clinical research funding from CARsgen Therapeutics, Celgene, Exelixis, Janssen Biotech, Sanofi-Aventis, Takeda Pharmaceuticals North America, Inc.: Research Funding; Amgen, Inc., AstraZeneca, BMS, Celgene, EcoR1 Capital LLC, Forma Therapeutics, Genzyme, GSK Biologicals, Ionis Pharmaceuticals, Inc., Janssen Biotech, Juno Therapeutics, Kite Pharma, Legend Biotech USA, Molecular Partners, Regeneron Pharmaceuticals, Inc.,: Honoraria, Membership on an entity's Board of Directors or advisory committees. Champlin:Takeda: Patents & Royalties; Genzyme: Speakers Bureau; DKMS America: Membership on an entity's Board of Directors or advisory committees; Cytonus: Consultancy; Actinium: Consultancy; Johnson and Johnson: Consultancy; Omeros: Consultancy. Qazilbash:Bioline: Research Funding; Janssen: Research Funding; Amgen: Research Funding; Bioclinica: Consultancy; Angiocrine: Research Funding.

This feature is available to Subscribers Only
Sign In or Create an Account Close Modal